


Introduction:
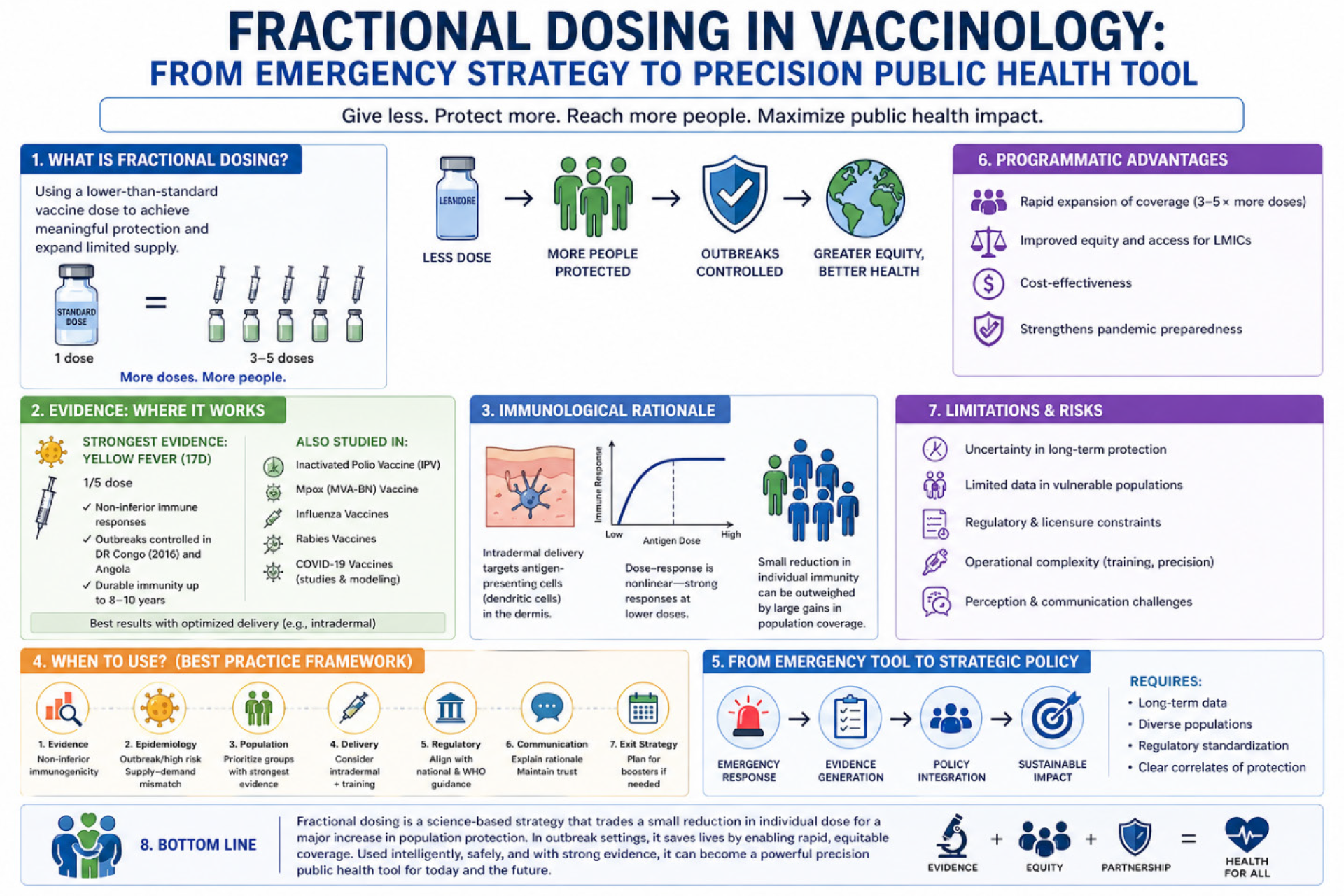
Fractional dosing—defined as the administration of a reduced quantity of antigen compared to the standard licensed dose—has evolved from a contingency approach into a credible, evidence-based public health strategy. Initially deployed during vaccine shortages, it is now increasingly recognized as a tool to expand coverage, improve equity, and optimize population-level impact.
This approach is grounded in a key immunological principle: vaccine dose–response relationships are often nonlinear. In many cases, a substantial proportion of the maximal immune response can be achieved at doses lower than the standard formulation. This creates an opportunity to trade small reductions in individual immunogenicity for large gains in population coverage, particularly critical in outbreak settings and supply-constrained environments.
Evidence Base: Where Fractional Dosing Works:
The most compelling evidence comes from Yellow Fever vaccination. Randomized trials and observational studies have consistently shown that administration of one-fifth of the standard 17D vaccine dose induces non-inferior neutralizing antibody responses in healthy adults.
Crucially, this evidence has been translated into real-world impact. During the 2016 Yellow Fever outbreak in Democratic Republic of the Congo, fractional dosing was implemented in Kinshasa as part of a mass vaccination campaign. Faced with limited global vaccine stockpiles, authorities used one-fifth doses to immunize millions of people in a short period. This strategy was instrumental in controlling the outbreak and is widely regarded as a landmark example of adaptive vaccinology in practice.
Similarly, fractional dosing has been used in outbreak responses in Angola during the same epidemic, further reinforcing its operational feasibility and public health value.
Long-term follow-up studies suggest that fractional doses can induce durable immunity, with high seroprotection rates reported up to 8–10 years. However, these data remain limited to specific populations and contexts and should be interpreted cautiously when extrapolating to broader use.
- Beyond Yellow Fever, fractional dosing has been explored in:
- Inactivated poliovirus vaccine (IPV).
- Mpox (MVA-BN) vaccine during recent outbreaks.
- Influenza and rabies vaccines.
- COVID-19 vaccines (immunogenicity and modeling studies).
- Malaria – RTS, S /AS01(E) vaccine.
Across these platforms, a consistent pattern emerges: fractional dosing can preserve immunogenicity, particularly when paired with optimized delivery routes such as intradermal administration.
The Immunological Rationale:
The dermis is highly enriched with antigen-presenting cells, particularly dendritic cells, making intradermal delivery especially efficient. This allows smaller quantities of antigen to generate robust immune responses.
In addition, correlates of protection—such as neutralizing antibody titers—often plateau at relatively low antigen doses. Modeling studies suggest that even modest reductions in individual-level protection may be outweighed by the benefits of increased population coverage, particularly during rapidly evolving outbreaks.
Programmatic Advantages:
Fractional dosing offers several strategic advantages:
- Rapid expansion of coverage:
Reducing the dose per vial can multiply available doses by 3–5 times, enabling rapid scale-up during outbreaks. - Equity and access:
This approach is particularly relevant for LMICs, where vaccine supply constraints remain a persistent challenge. - Cost-effectiveness:
Lower antigen requirements reduce costs per immunized individual, improving sustainability. - Pandemic preparedness:
Fractional dosing may play a critical role in early outbreak response, when supply is limited and speed is essential.
Limitations and Risks:
Despite its promise, fractional dosing is not universally applicable and carries important limitations:
- Uncertainty in long-term protection:
While Yellow Fever data are reassuring, the duration of immunity after fractional dosing remains insufficiently characterized for many vaccines. In outbreak settings, the primary goal is rapid short-term protection; however, there is a legitimate risk that reduced doses may not confer the same longevity of immunity as full-dose schedules. This raises important considerations for future booster strategies and long-term disease control. - Population variability:
Most evidence is derived from healthy adult populations. Data in infants, older adults, and immunocompromised individuals remain limited. - Regulatory constraints:
Fractional dosing is often implemented under emergency use frameworks rather than routine licensure. - Operational complexity:
Intradermal administration requires training and precision, increasing the risk of administration errors. - Perception and communication challenges:
Reduced-dose strategies may be perceived as inferior, potentially affecting public confidence if not communicated effectively.
When Should Fractional Dosing Be Used?
A rational framework for implementation includes:
1. Evidence threshold:
- Demonstrated non-inferior immunogenicity.
- Preferably supported by clinical trials or robust real-world data.
2. Epidemiologic context:
- Active outbreak or high transmission risk.
- Clear mismatch between supply and demand.
3. Target population:
- Prioritize groups with strongest evidence (typically healthy adults).
- Exercise caution in high-risk populations.
4. Delivery strategy:
- Consider intradermal administration when supported by evidence.
- Ensure adequate training of healthcare workers.
5. Regulatory alignment:
- Coordinate with national authorities and WHO guidance.
6. Communication strategy:
- Clearly explain the rationale to maintain trust.
7. Exit strategy:
- Plan for potential boosters if long-term protection is uncertain.
From Emergency Tool to Strategic Policy:
The success of fractional dosing in Yellow Fever outbreaks has demonstrated that this approach is not merely theoretical, but operationally feasible at scale.
The next challenge is determining whether fractional dosing should remain an emergency measure or evolve into a proactive, evidence-based strategy within routine immunization and pandemic preparedness frameworks.
This will require:
- Expanded long-term immunogenicity data.
- Inclusion of diverse populations.
- Regulatory standardization.
- Clear correlates of protection.
Conclusions:
Fractional dosing represents a shift in vaccinology—from a scarcity-driven compromise to a potentially optimized strategy for maximizing population health impact.
However, its use must remain context-specific and evidence-driven. In outbreak settings, the benefits of rapid, expanded coverage are clearly demonstrated in Yellow Fever epidemics. Yet, the potential trade-off in long-term immunity underscores the need for careful planning, follow-up strategies, and ongoing research.
In a world of constrained resources and emerging threats, the critical question is not whether fractional dosing works—but how to deploy it intelligently, safely, and sustainably.
Bibliography:
- Roukens AHE, Visser LG. Fractional-dose yellow fever vaccination: an expert review. J Travel Med. 2019 Sep 2;26(6):taz024. doi: 10.1093/jtm/taz024.
- Juan-Giner A, Kimathi D, Grantz KH, Hamaluba M, Kazooba P, Njuguna P, Fall G, Dia M, Bob NS, Monath TP, Barrett AD, Hombach J, Mulogo EM, Ampeire I, Karanja HK, Nyehangane D, Mwanga-Amumpaire J, Cummings DAT, Bejon P, Warimwe GM, Grais RF. Immunogenicity and safety of fractional doses of yellow fever vaccines: a randomised, double-blind, non-inferiority trial. Lancet. 2021 Jan 9;397(10269):119-127. doi: 10.1016/S0140-6736(20)32520-4.
- World Health Organization. WHO position on the use of fractional doses – June 2017, addendum to vaccines and vaccination against yellow fever WHO: Position paper – June 2013. Vaccine. 2017 Oct 13;35(43):5751-5752. doi: 10.1016/j.vaccine.2017.06.087.
- Wilder-Smith A, Barrett A, Vannice K, Hombach J. Long-Term Protection After Fractional-Dose Yellow Fever Vaccination. Ann Intern Med. 2019 Jul 16;171(2):145-146. doi: 10.7326/L19-0196.
- Resik S, Tejeda A, Sutter RW, Diaz M, Sarmiento L, Alemañi N, Garcia G, Fonseca M, Hung LH, Kahn AL, Burton A, Landaverde JM, Aylward RB. Priming after a fractional dose of inactivated poliovirus vaccine. N Engl J Med. 2013 Jan 31;368(5):416-24. doi: 10.1056/NEJMoa1202541.
- Schnyder JL, De Pijper CA, Garcia Garrido HM, Daams JG, Goorhuis A, Stijnis C, Schaumburg F, Grobusch MP. Fractional dose of intradermal compared to intramuscular and subcutaneous vaccination – A systematic review and meta-analysis. Travel Med Infect Dis. 2020 Sep-Oct;37:101868. doi: 10.1016/j.tmaid.2020.101868.
- Nelson KS, Janssen JM, Troy SB, Maldonado Y. Intradermal fractional dose inactivated polio vaccine: a review of the literature. Vaccine. 2012 Jan 5;30(2):121-5. doi: 10.1016/j.vaccine.2011.11.018.
- Du Z, Liu C, Bai Y, Wang L, Lim WW, Lau EHY, Cowling BJ. Predicting Efficacies of Fractional Doses of Vaccines by Using Neutralizing Antibody Levels: Systematic Review and Meta-Analysis. JMIR Public Health Surveill. 2024 Jul 12;10:e49812. doi: 10.2196/49812.
- Chen Z, Liu K, Liu X, Lou Y. Modelling epidemics with fractional-dose vaccination in response to limited vaccine supply. J Theor Biol. 2020 Feb 7;486:110085. doi: 10.1016/j.jtbi.2019.110085.
- WHO. Mpox vaccine fractional dosing guidance. 2025. chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://cdn.who.int/media/docs/default-source/immunization/mpox/who_faq_intradermal_fractional_dosing_mva-bn_vaccine.pdf?sfvrsn=ab124257_3&utm_source=chatgpt.com.
- Yang B, Huang X, Gao H, Leung NH, Tsang TK, Cowling BJ. Immunogenicity, efficacy, and safety of SARS-CoV-2 vaccine dose fractionation: a systematic review and meta-analysis. BMC Med. 2022 Oct 25;20(1):409. doi: 10.1186/s12916-022-02600-0.
- Osei-Tutu L, Kariuki SK, Lee CK, Fabre R, Bii DK, Adjei S, Oneko M, Attobrah Sarfo MA, Ockenhouse CF, Schuerman L, Buabeng PBY, Bakari A, Atieno C, Kotoh-Mortty MF, Otieno K, Ntiamoah Y, Sang T, Bollaerts A, Westercamp N, Ansong D, Agbenyega T, Samuels AM, Ofori-Anyinam O; RTS,S study group. Sustained efficacy of the RTS,S/AS01E malaria vaccine over 50 months of follow-up when used in full-dose or fractional-dose regimens in young children in Ghana and Kenya: final results from an open-label, phase 2b, randomised controlled trial. Lancet Glob Health. 2025 Oct;13(10):e1723-e1736. doi: 10.1016/S2214-109X(25)00272-4.
- Westercamp N, Osei-Tutu L, Schuerman L, Kariuki SK, Bollaerts A, Lee CK, Samuels AM, Ockenhouse C, Bii DK, Adjei S, Oneko M, Lievens M, Attobrah Sarfo MA, Atieno C, Bakari A, Sang T, Kotoh-Mortty MF, Otieno K, Roman F, Buabeng PBY, Ntiamoah Y, Ansong D, Agbenyega T, Ofori-Anyinam O. Could Less Be More? Accounting for Fractional-Dose Regimens and Different Number of Vaccine Doses When Measuring the Impact of the RTS,S/AS01E Malaria Vaccine. J Infect Dis. 2024 Aug 16;230(2):e486-e495. doi: 10.1093/infdis/jiae075.
- Sinilaite A, Doyon-Plourde P, Young K, Harrison R. Summary of the National Advisory Committee on Immunization (NACI) Statement-Recommendations on Fractional Influenza Vaccine Dosing in the Event of a Shortage: Pandemic preparedness. Can Commun Dis Rep. 2023 Apr 1;49(4):90-98. doi: 10.14745/ccdr.v49i04a01.
- Roozen GVT, Prins MLM, van Binnendijk R, den Hartog G, Kuiper VP, Prins C, Janse JJ, Kruithof AC, Feltkamp MCW, Kuijer M, Rosendaal FR, Roestenberg M, Visser LG, Roukens AHE. Safety and Immunogenicity of Intradermal Fractional Dose Administration of the mRNA-1273 Vaccine: A Proof-of-Concept Study. Ann Intern Med. 2022 Dec;175(12):1771-1774. doi: 10.7326/M22-2089. Epub 2022 Oct 25.




")
{kind=link}