


Introduction:
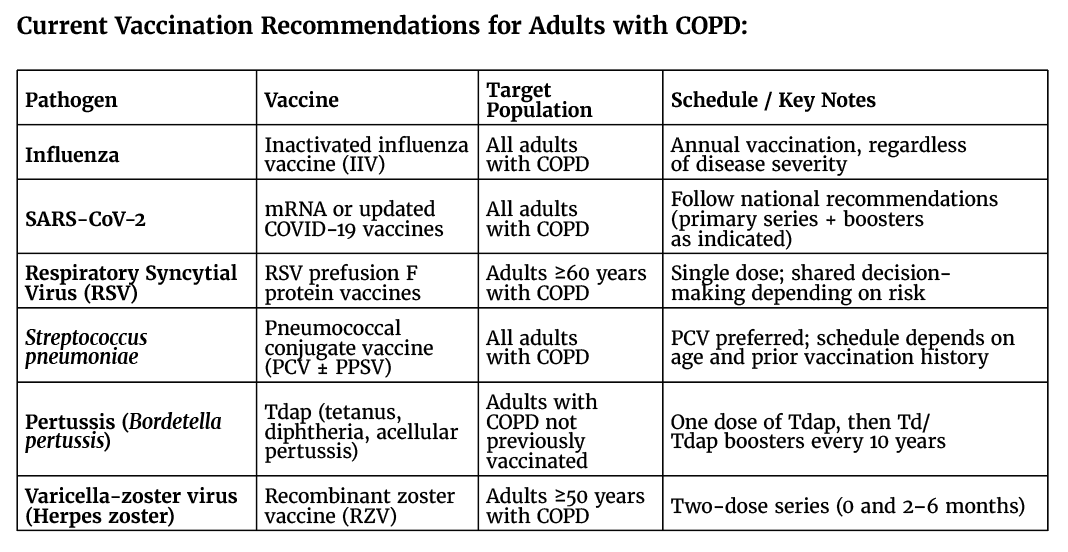
Chronic obstructive pulmonary disease (COPD) is highly susceptible to infectious triggers, with respiratory viruses and bacteria playing a central role in precipitating acute exacerbations. These events are major drivers of disease progression, healthcare utilization, and mortality. Preventing infection is therefore a cornerstone of COPD management, positioning vaccination as a key intervention to reduce exacerbations and improve clinical outcomes. Current recommendations from the Global Initiative for Chronic Obstructive Lung Disease (GOLD) emphasize immunization against influenza, Streptococcus pneumoniae, respiratory syncytial virus (RSV), severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), pertussis, and varicella-zoster virus. This month’s Best Practice section summarizes contemporary vaccination strategies in adult patients with COPD and examines the evidence supporting their clinical benefits.
Increased susceptibility to respiratory pathogens in adults with COPD:
Adults with COPD have increased susceptibility to respiratory infections due to impaired mucociliary clearance, chronic airway inflammation, structural lung damage, and both innate and adaptive immune dysfunction. These alterations facilitate airway colonization and reduce the ability to clear pathogens effectively. As a result, COPD patients are particularly vulnerable to infections caused by Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis, influenza virus, respiratory syncytial virus (RSV), and SARS-CoV-2. Viral infections may also predispose to secondary bacterial infections, further amplifying disease severity. This heightened susceptibility contributes to more frequent and severe exacerbations, accelerated lung function decline, increased healthcare utilization, and higher mortality.
Influenza:
Influenza remains a major respiratory pathogen, contributing substantially to morbidity, mortality, and healthcare burden worldwide. Recent estimates in the United States alone report millions of cases, with hundreds of thousands of hospitalizations and thousands of deaths occurring within a single influenza season.
In patients with COPD, influenza infection is a well-recognized trigger of acute exacerbations, often resulting in severe clinical outcomes, including hospitalization, respiratory failure, and increased mortality. The underlying mechanisms include heightened airway inflammation, impaired immune responses, and enhanced susceptibility to bacterial colonization, all of which amplify disease severity. In addition, COPD is associated with systemic inflammation, reflected by elevated circulating inflammatory markers, which contributes to a high burden of comorbid conditions. Notably, acute exacerbations are frequently accompanied by cardiovascular complications, further increasing the risk of adverse outcomes.
Given this interplay between influenza and COPD exacerbations, prevention is a critical component of disease management. Annual influenza vaccination is strongly recommended for all patients with COPD, regardless of disease severity, and represents a cost-effective strategy to reduce exacerbations, hospitalizations, and overall healthcare utilization.
Respiratory Syncytial Virus (RSV):
Respiratory syncytial virus (RSV) is an important cause of respiratory illness, ranging from mild upper respiratory infections to severe lower respiratory tract disease, including bronchiolitis and pneumonia. While traditionally associated with pediatric populations, RSV also poses a substantial risk to older adults and individuals with chronic conditions such as COPD.
In this population, RSV contributes meaningfully to disease burden, accounting for a notable proportion of acute exacerbations and leading to significant outpatient visits, hospitalizations, and mortality worldwide. The risk of severe disease increases with age, partly due to immunosenescence and diminished RSV-specific cellular immune responses, resulting in more severe and prolonged illness.
Management of RSV infection remains largely supportive; however, prevention has advanced considerably with the development of effective vaccines. Current recommendations advise RSV vaccination for adults with COPD beginning at 60 years of age. Available vaccines target the viral fusion (F) glycoprotein, a key mediator of viral entry, enabling protection against both RSV subtypes (A and B).
Recent large clinical trials have demonstrated that RSV vaccines provide high levels of protection against lower respiratory tract disease, severe illness, and acute respiratory infections, with efficacy generally ranging from approximately 65% to over 90%. These findings, as well as real-life evidence, position RSV vaccination as a critical strategy to reduce disease burden and improve outcomes in patients with COPD.
SARS-CoV-2:
The COVID-19 pandemic has posed substantial challenges worldwide, with disproportionate impact on individuals with chronic respiratory diseases such as COPD. These patients, characterized by impaired lung function, chronic inflammation, and frequent exacerbations, are particularly vulnerable to respiratory infections. Infection with SARS-CoV-2 can result in severe complications, including pneumonia, acute respiratory distress syndrome, and multi-organ failure, leading to higher rates of hospitalization, intensive care utilization, and mortality among patients with COPD.
Vaccination has emerged as a cornerstone in mitigating these risks, with COVID-19 vaccines demonstrating strong effectiveness in preventing severe disease and adverse outcomes. Accordingly, vaccination is strongly recommended for individuals with COPD in line with national guidelines.
In parallel, non-pharmaceutical interventions implemented during the pandemic—such as masking, physical distancing, and stay-at-home measures—were associated with a marked reduction in respiratory viral transmission. Notably, these measures coincided with a substantial decline in hospitalizations for COPD exacerbations, underscoring the central role of viral infections in driving disease instability and highlighting the importance of preventive strategies in this population.
Herpes zoster:
Herpes zoster, caused by reactivation of latent varicella-zoster virus, occurs more frequently in individuals with chronic conditions such as COPD, with potentially increased risk among those receiving inhaled corticosteroids. Beyond its acute dermatologic manifestations, herpes zoster can lead to post-herpetic neuralgia, a debilitating complication associated with persistent pain and reduced quality of life.
In patients with COPD, herpes zoster is also associated with increased healthcare utilization and higher costs, reflecting its broader clinical and economic impact. Preventive strategies are therefore essential in this population.
Vaccination against varicella-zoster virus has been shown to significantly reduce the incidence of herpes zoster and its complications. Current recommendations support vaccination in adults with COPD aged 50 years and older. Evidence indicates that the recombinant zoster vaccine substantially lowers the risk of both mild and severe disease, while additional data suggest potential cardiovascular benefits, including reduced risks of myocardial infarction and stroke in individuals with chronic diseases.
Streptococcus pneumoniae:
In addition to viral pathogens, bacterial infections play a major role in COPD morbidity. Among these, Streptococcus pneumoniae is a leading cause of pneumonia and invasive disease, contributing substantially to hospitalization and mortality. COPD patients are particularly susceptible due to impaired mucociliary clearance, chronic airway inflammation, and structural lung damage, which facilitate bacterial colonization and infection.
Episodes of pneumococcal pneumonia often initiate a cascade of adverse outcomes. Following community-acquired pneumonia, patients with COPD have a higher risk of subsequent exacerbations, reflecting a cycle of worsening lung injury, functional decline, and increased vulnerability to future infections. Recurrent exacerbations further impair host defenses, promoting persistent colonization and accelerating disease progression.
Vaccination is a key strategy to interrupt this cycle. Two main types of pneumococcal vaccines are available: polysaccharide and protein-polysaccharide conjugate vaccines, both targeting capsular polysaccharides of disease-causing serotypes. Current recommendations favor the use of pneumococcal conjugate vaccines in patients with COPD due to their enhanced immunogenicity and broader clinical benefits.
Pertussis:
Pertussis, or whooping cough, is a highly contagious respiratory infection caused by Bordetella pertussis. Although often underrecognized in adults, it represents a relevant risk for individuals with COPD, who are more susceptible to respiratory infections due to impaired airway defenses and chronic inflammation. In this population, pertussis infection may lead to prolonged cough, increased frequency of exacerbations, and greater healthcare utilization, including longer hospital stays.
Importantly, COPD does not appear to impair the immunogenicity of pertussis vaccination. Studies indicate that patients with COPD are capable of mounting robust immune responses following vaccination, characterized by activation of T-follicular helper cells, expansion of plasmablasts, and production of specific antibodies. These findings support the effectiveness of vaccination in this high-risk group.
Given the potential clinical impact of pertussis and the demonstrated vaccine responsiveness, immunization is a key preventive strategy. Current recommendations advise that adults with COPD who have not previously been vaccinated receive the reduced-antigen-content diphtheria-tetanus-acellular pertussis (Tdap) vaccine, consistent with broader adult immunization guidelines.
Conclusions:
Respiratory infections remain a major driver of morbidity, exacerbations, and mortality in adults with COPD, underscoring the critical role of vaccination as a cornerstone of disease management. Immunization against key pathogens—including influenza, pneumococcus, SARS-CoV-2, RSV, pertussis, and varicella-zoster virus—has demonstrated clear benefits in reducing disease burden, preventing complications, and improving clinical outcomes.
Despite strong evidence and consistent guideline recommendations, adult vaccination coverage remains suboptimal worldwide. Barriers such as limited awareness, fragmented healthcare delivery, access constraints, and vaccine hesitancy continue to impede effective implementation. These challenges are further amplified by inequities in vaccine access across regions and populations, leaving many high-risk individuals insufficiently protected.
Addressing these gaps requires a coordinated, multi-level approach that prioritizes vaccine equity, strengthens healthcare system integration, and promotes routine adult immunization as a standard of care. Improving coverage in adults—particularly those with chronic conditions such as COPD—remains a critical yet underachieved public health objective.
Advancing vaccination strategies in this population will depend not only on continued innovation in vaccine development, but also on more effective implementation, equitable access, and sustained efforts to increase uptake. Ultimately, closing the gap between recommendations and real-world coverage is essential to fully realize the benefits of vaccination in COPD.
References:
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: 2024 report. GOLD; 2024. https://goldcopd.org/2024-gold-report/.
- Venkatesan P. GOLD COPD report: 2024 update. Lancet Respir Med. 2024;12(1):15–16. doi:10.1016/S2213-2600(23)00461-7.
- Falsey AR, Hennessey PA, Formica MA, Cox C, Walsh EE. Respiratory syncytial virus infection in elderly and high-risk adults. N Engl J Med. 2005;352(17):1749–59. doi:10.1056/NEJMoa043951.
- Cunningham AL, Lal H, Kovac M, Chlibek R, Hwang SJ, Díez-Domingo J, et al. Efficacy of the herpes zoster subunit vaccine in older adults. N Engl J Med. 2016;375(11):1019–32. doi:10.1056/NEJMoa1603800.
- Thompson MG, Stenehjem E, Grannis S, Ball SW, Naleway AL, Ong TC, et al. Effectiveness of COVID-19 vaccines in ambulatory and inpatient care settings. N Engl J Med. 2021;385(15):1355–71. doi:10.1056/NEJMoa2110362.
- Goeijenbier M, van Sloten TT, Slobbe L, Mathieu C, van Genderen P, Beyer WE, et al. Benefits of influenza vaccination for patients with COPD: a systematic review. Vaccine. 2017;35(26):3430–7. doi:10.1016/j.vaccine.2017.05.005.
- Torres A, Cilloniz C, Blasi F, Chalmers JD, Gaillat J, Dartois N, et al. Burden of pneumococcal community-acquired pneumonia in adults: a literature review. Respir Med. 2018;137:6–13. doi:10.1016/j.rmed.2018.02.003.
- McElhaney JE, Andrew MK, McNeil SA. Estimating influenza vaccine effectiveness in older adults. Vaccine. 2021;39(25):3309–15. doi:10.1016/j.vaccine.2021.04.055.
- Klein NP, Fireman B, Yih WK, Lewis E, Kulldorff M, Ray P, et al. Surveillance for adverse events after COVID-19 mRNA vaccination. JAMA. 2021;326(14):1390–9. doi:10.1001/jama.2021.15072.
- Patel N. An update on COPD prevention, diagnosis, and management: The 2024 GOLD Report. Nurse Pract. 2024 Jun 1;49(6):29-36. doi: 10.1097/01.NPR.0000000000000180.
- Kwok W-C, Wong J-NC, Cheung A, Tam TC-C. Vaccination in Chronic Obstructive Pulmonary Disease. Vaccines. 2025; 13(3):218. https://doi.org/10.3390/vaccines13030218.
- Porto Fuentes Ó, Muela Molinero A, Alonso Ortiz MB. Vaccination in chronic obstructive pulmonary disease (COPD): Scientific evidence and strategies to reduce risks. Rev Clin Esp (Barc). 2025 Aug-Sep;225(7):502330. doi: 10.1016/j.rceng.2025.502330.




")
{kind=link}